
Exporteer av AGA’s AutoChemist tot UML, United Medical Laboratory in Portland Oregon som är VS: s största privatägda laboratorium för leverans av kemiska analysresultat till privatläkare och sjukhus över hela USA. En ny unik exportmarknad har öppnats för svensk elektromedicinsk industri riktad mot det snabbast expanderande marknadsområdet inom USA.







The History of the AutoChemist®:
From Vision to Reality
H. E. Peterson, I. Jungner
Stockholm, Sweden
1 Introduction
The largest clinical analyzer system created
for clinical laboratories, called the AutoChemist, was developed in the mid-1960s
and used until the late 1980s. Its development
started when Gunnar Jungner, MD, PhD,
Associate Professor in Clinical Chemistry at
the University of Gothenburg, Sweden, was
a Visiting Scientist at the National Institute of
Health (NIH) in the US. He became a member
of a team working on the automation of hospital laboratories at the Department of Clinical
Pathology, Clinical Center, which was headed
by Dr George Z Williams [1-5]. Another
notable member of the working team was
Earnest Cotlove [6-7]. Ingmar Jungner, MD
PhD, a younger brother of Gunnar Jungner,
visited NIH at the autumn 1959 and and took
part of their plans to make the laboratory work
more efficient through the use of laboratory
robots and by directing their work towards
an automated hospital laboratory through an
“electronic brain”. An unforgettable event
during his stay was a visit together with the
working team to the aircraft manufacturer
Boeing, whom NIH had commissioned
to construct an automated blood analyzer.
The project was lead by Jordan J Baruch, a
genial technical consultant for NIH [8]. In
1966, Dr Williams, Dr Cotlove, Mr Baruch,
and Gunnar Jungner presented the results of
their work at the International Conference on
Automated Data Processing in Hospitals in
Elsinore (Denmark) [9-13].
2 History of the AutoChemist
The Start – 1960
When Gunnar Jungner returned to Sweden,
he created interest in the improvement of laboratory performance in Sweden. The Swedish Agency for Health Services Development
(SJURA) appointed Gunnar Jungner as the
President of their working group on Clinical Chemistry. Hence, the Jungner brothers
started to improve laboratory efficiency
using tempo-automation and automation of
single analyses. In parallel they developed
a multi-channel equipment for large-scale
health screening, which later resulted in the
Värmland equipment [13-15].
The Värmland Survey
Following the initiative of the Jungner brothers, Swedish authorities decided in 1962 to
apply on a large scale chemical analysis in
the county of Värmland (300 kilometres
northwest of Stockholm). 100,000 persons
older than 25 years were screened from late
1962 to late 1964 [13-20] with a battery
of twelve blood analyses. The apparatus
system used in the project was built by the
Jungner brothers [13-15]. More than one
million analyses were performed during this
two-year period. For the Jungner brothers,
the Värmland project was an incentive to
continue the technical development. It was
rather challenging for two years when several
hundred blood specimens were arriving for
processing at the Stockholm laboratory by
the night train from Karlstad four to five days
a week. Every time the home-grown system
was in a crisis, there were discussions about
how to construct a safer installation.
Hospital for Infectious Diseases
Project (SJURA 404)
A project for hospital automation was also
initiated with the support of SJURA [21-23].
The Jungner brothers in collaboration with
Hans Peterson, MD PhD [23] realised thatthere was a need for a hospital service, a
service whereby automated units (i.e. wards,
laboratories, storage facilities, etc.) could be
connected through telecommunication and
the automated transport of material. They
considered hospital wards and other clinical
entities as consumers demanding support
from their service departments and identified
the need for a communication system to
provide clinical information and material.
However, to automate this communication,
consumer and service units needed to be
equipped with in- and out-functions.
At the Hospital for Infectious Diseases
(Stockholm, Sweden), where Ingmar Jungner headed the Chemistry Department,
our team started in 1964 a project with an
automated requisition and report system
[12] adapted to a teletypewriter as an inand output unit, an order box for simple
requisition and a patient record system for
the reports produced. The referral contained
patient identification information and a short
summary of the case history together with information about the laboratory requisitions.
The requisition was sent to the laboratory
via the order box, from where reports were
then returned to the wards with information
on date and lab results. A paper printout
was produced to fit patient’s medical records
allowing easy access for clinicians. Moreover, small cards were produced providing
a summary of all relevant clinical information for health professionals to optimise
patient management. The teletypewriter
was equipped with a reader and a punch for
an eight-channel paper tape approved for
connection to the regular telephone network.
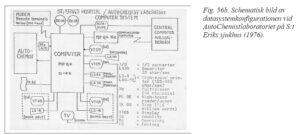
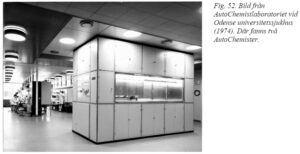
The AutoChemist System at the
Hospital for Infectious Diseases
The AutoChemist System used at the Hospital for Infectious Diseases was constructed
around a large multiple robot analyzer (Fig.
1), wherein one central unit could execute
up to 40 different analytical methods (Fig.
2). Special connected measuring stations
(satellite stations) were available for those
analyses not suitable for full automation.
The system was computer-based and worked
online through a connection with the central
unit and a telecommunication system. This
system provided an automated requisition
and reporting system using the previously
described teletypewriters as well as boxes. These boxes were connected with the
teletype of the ward which allowed correct
identification of patients by room and bed.
The teletype and its connected cables
allowed a simple push-button to provide the
correct identification details for a patient,
automatically extracted from the computer
memory. The push-button of the Order box
then allowed requesting of the appropriate
analyses from the relevant laboratory and/
or examination. This information was also
sent to the laboratory computer, which then
received data to print out an order form for
the right requisition (e.g. sample taking). A
requisition could easily be extended through
manual input on the teletypewriter.
Computerisation and Software
Development for the Hospital for
Infectious Diseases
The technical developments of the
AutoChemist continued after 1964, but
the greatest improvements came from
information technology. Until then, computers were not available for standard use,
as they were considered too progressive
and too expensive for the market and small
data units were still under development.
Eurocomp LGP 21, a German manufactured minicomputer, was used along with a
prototype of the AutoChemist. At that time, core memories were not in use yet and cycle
times were measured in milliseconds rather
than in microseconds. Further improvements
were thus required to obtain an access time
between 8 and 41 milliseconds. However,
one still had to add the time needed to perform the tasks. The AutoChemist delivered
20 reports every 20 seconds. As a result, the
time required to read the value on a digital
voltmeter was too long. This problem was
temporarily solved by manually inserting
every second instruction diagonally on the
disc, thus achieving twice the speed.
The LGP 21 was then replaced by a
Digital Equipment Corporation’s PDP-5,
which was equipped with core storage, a
programme controlled Multiplexer, an A/D
converter and a double magnetic tape station,
which was shown to be very useful for the
telecommunication system in the hospital.
Computer development was accelerating
[24] and in 1965 Digital presented its first
mass-produced mini computer PDP-8 [25].
At this time, the software rather than the
hard ware became a problem for the further
enhancement of the AutoChemist. In 1965,
a relatively simple programme, MACH –
Main Program, was developed to handle all
procedures of the AutoChemist [26].
The Development of the Mass
Analyzer AutoChemist – the First
Automated and Computerised
Multichannel Analyzer (1965)
The previously described Värmland project
[13-20] encouraged the Jungner brothers
to continue the technical development of
the AutoChemist. Repeated failures of the
home-grown system revealed the need
for a safer installation of mass analyses
based on new ideas and technical solutions,
without abandoning existing techniques.
This required a system with high capacity,
versatility, and compactness, but easy maintenance and low labour-intensity. This thus
called for automated printing under minimal
supervision. The existing equipment at that
time did not respond to the high degree of
mechanising needed to provide an essential
advance in laboratory automation. The
demand for an industrial production of analyses and reagents was the subject of
multiple debates in the field of biochemistry,
and the task was theoretically possible since
the pharmaceutical industry had already
provided pipetted fluids for many years. The
Jungner brothers and their team realised that
automation needed to allow the processing
of a large number of different analytical
procedures whereby different specimens,
including whole blood, serum, urine, cerebrospinal fluid or extract, were analysed
simultaneously. They estimated that 20 to 40
different analyses of a much larger quantity
were required, thus highlighting the need for
a computerised mass analyzer.
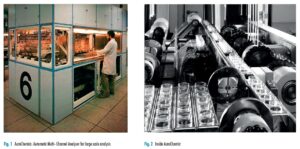
Creating a Prototype
As a consequence, a prototype was created by the lab’s own staff involving two
instrument makers and about ten volunteer
medical students. The resulting device was
enormous as the installation was four meters
long. It was two meters high and two meters
wide (Fig. 1). This size was necessary to
allow the transportation of thousands of
centrifuge tubes (samples) in heavy metal
racks hanging on motorcycle chains, supported by very thick beams (Fig.2). With
a capacity of 3,000 to 6,000 analyses per
hour, pneumatic pipettes (see below), and an
integrated computer, the AutoChemist was
unique and the largest of its kind. This first
AutoChemist was manufactured by AGA,
Lidingö, Sweden.
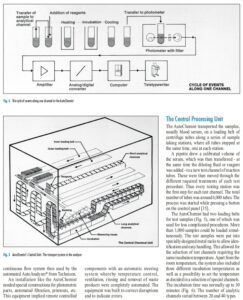
3 Technical Specifications of
the AutoChemist
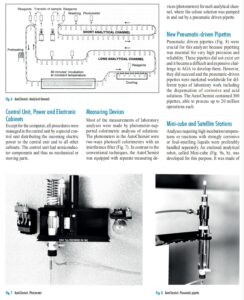
The Operating System of the
AutoChemist Figure 3 depicts the operating system of the
analyzer and Figure 4 illustrates the analyses
occurring in one channel of the AutoChemist. Since the AutoChemist was mechanical
[27-34], reagents were added by pipettes
and transported with the sample within each
analysis channel whereby a chain system
was transported through the right incubation temperatures. The vertical movement
allowed for changeable dimensions with
sufficient reaction time at high analysis
speed. All specimens and reagent mixtures
were handled to avoid contamination of test
samples, a technique called “discrete sample
handling” which was in contrast with the continuous flow system then used by the
automated AutoAnalyzer® from Technicon.
An installation like the AutoChemist
needed special constructions for photometric
parts, automated filtration, printouts, etc.
This equipment implied remote controlled components with an automatic steering
system whereby temperature control,
ventilation, rinsing and removal of waste
products were completely automated. The
equipment was built to correct disruptions
and to indicate errors. The Central Processing Unit
The AutoChemist transported the samples,
usually blood serum, on a loading belt of
centrifuge tubes along a series of sample
taking stations, where all tubes stopped at
the same time, one at each station.
A pipette drew a calibrated volume of
the serum, which was then transferred – at
the same time the diluting fluid or reagent
was added – to a new test channel of reaction
tubes. These were then moved through the
different required treatments of each test
procedure. Thus every testing station was
the first step for each test channel. The total
number of tubes was around 6,000 tubes. The
process was started while pressing a button
on the control panel [35].
The AutoChemist had two loading belts
for test samples (Fig. 5), one of which was
used for less complicated procedures. More
than 1,000 samples could be loaded simultaneously. The test samples were put into
specially designed metal racks to allow identification and easy handling. This allowed for
the selection of test channels requiring the
same incubation temperature. Apart from the
room temperature, the system also included
three different incubation temperatures as
well as a possibility to set the temperature
as decided in a selection of special channels.
The incubation time was normally up to 30
minutes (Fig. 6). The number of analytic
channels varied between 20 and 40 types.Control Unit, Power and Electronic
Cabinets
Except for the computer, all procedures were
managed in the central unit by a special control unit distributing the incoming electric
power to the central unit and to all other
cabinets. The control unit had semiconductor components and thus no mechanical or
moving parts.Measuring Devices
Most of the measurements of laboratory
analyses were made by photometer-supported colorimetric analyses of solutions.
The photometers in the AutoChemist were
two-ways photocell colorimeters with an
interference filter (Fig. 7). In contrast to the
conventional techniques, the AutoChemist
was equipped with separate measuring de
vices (photometers) for each analytical channel, where the colour solution was pumped
in and out by a pneumatic driven pipette.
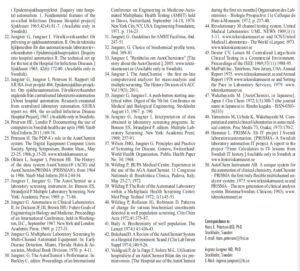
New Pneumatic-driven Pipettes
Pneumatic driven pipettes (Fig. 8) were
crucial for this analyzer because pipetting
was essential for very high precision and
reliability. These pipettes did not exist yet
and it became a difficult and expensive challenge to AGA to develop them. However,
they did succeed and the pneumatic-driven
pipettes were marketed worldwide for different types of laboratory work including
the dispensation of corrosive and acid
solutions. The AutoChemist contained 300
pipettes, able to process up to 20 million
operations each.
Mini-cube and Satellite Stations
Analyses requiring high incubation temperatures or reactions with strongly corrosive
or foul-smelling liquids were preferably
handled separately. An enclosed analytical
robot, called Mini-cube (Fig. 9a, b), was
developed for this purpose. It was made ofa corrosion safe material and could be enclosed in the central unit where there was
room for four such cubes. The incubation
temperature could be set up to 110 degrees
Celsius. One advantage of the automated
laboratory was that it could connect to other
activities within or outside the laboratory
through other satellite stations. This satellite (Fig. 10) could even be a station for a
completely different measuring instrument,
directly attached to the AutoChemist computer. It could provide assistance in analytic
measurements, corrections, and controls,
as well as use the same requisition and
reporting system of automatic analyses. As
a result, hospital wards were in a way also
in- and output satellite stations.
Computer, Software, Registration,
and Printout
In the project at the Hospital for Infectious
Diseases, a more sophisticated program
than the already existing MIACH 3 was
developed for the AutoChemist [26]. At
the hospital, the analyzer was supported
by a PDP-8 computer and an ASR Teletype
Writer teleprinter. In 1975, an upgrade of the
software was released, the MIACH 4 with a
Quality Control Program, which soon after
became the MIACH 5 [26] (See Fig. 11).
Gradually MIACH 4 became the skeleton of a further development whereby the
AutoChemist was incorporated in an entire
computer system for clinical laboratories and the new PDP-12 computer from Digital
Equipment [26]. The resulting new system,
called the Clinical Laboratory System
(CLACH), made the AutoChemist adaptable to any laboratory system. It became a
flexible, independent, and easily modifiable
system that could be extended to 8K cores.
As the software was written in sections, it
provided the possibility for CLACH to be used with two computers to meet the high
demand for reliability in a real-time system.
The AutoChemist was preliminary designed for photometric determination and
registration of the analytic results. The measurement data from each test sample were
converted to digital values and stored in the
computer. When all the measurements of the
patient had been made, the test results were printed out, collected, checked and punched
to be stored for further data analyses.
The demands on the computer system
were steadily increasing [26]. It was necessary to complete and introduce age/gender
information to analytical results, printed in
different columns for normal, slightly or
strongly deferring results. Automatic corrections of all analyses and comments on
the results, according to generally accepted
guidelines, were also introduced.
Industrial Reagent Manufacturing
This multi-channel analyzer used reagents
in volumes that were not seen before. In
the early 1960s, it was common practice for
laboratories to produce their own reagents in
volumes of a few litres (L), but negotiations
with chemical manufacturers resulted in the
industrial production of reagents on a larger
scale providing easy transportable containers
for up to a-month storage. A 25L-container,
easy to transport and handle, became a
standard.
Analyses Programmes
The possibility to analyse different materials
simultaneously was very important. The
AutoChemist could for instance analyse
blood serum on the outer belt and urine on
the inner belt. One could thus chose an analytic combination representing a programme
for serum involving more than 20 different
types of analyses as well as a programme for
urine. This then fulfilled the requirements for
a variety of medical procedures including
hospital analyses and health screening [14,
15, 32, 36]. The result was the introduction
of ”Chemical Health Screening”. Chemical
analyses of blood and urine were conducted
to search for signs of illness (pathological
changes). These screening tests could be
performed as part of health check-ups, which
could also include other medical procedures
such as X-rays, or as part of a screening
procedure for healthy individuals to identify
those, who may need treatment [37].
Chemical Health Screening for the asymptomatic population thus provides many
advantages: • Changes in blood usually appear before
clinical symptoms arise
• Many clinical symptoms can often easily
be explained by metabolic disturbances,
which can be identified in the blood
• Blood serum is easy to take, also in primitive situations and on a large scale
• Blood serum can be long lasting and
transported long distance for analysis
• Blood serum can be analysed on a large
scale by robot analyzers
• A large number of analyses on each sample increases the medical value
• Analytical results can be processed by a
computer or are readable through inexpensive mechanical methods
Analytical Capacity
The maximal test capacity in the first basic
version of the AutoChemist was 135 samples
per hour for each belt. This corresponded to
an analytical capacity of 24 channels of at
least 3,000 analyses per hour. An adequate
margin for standard tests, calibration, emergency tests was included and the amount of
channels was increased by driving two belts
and/or using additive equipment such as
mini-cubes, flame photometers, or fluorimeters. This doubled the analysing capacity
to 6,000 analyses per hour, which was ten
times more than the Värmland project implemented only a few years earlier (Fig. 12).
Thus, a full eight-hour shift with 24 channelscould provide a production of seven million
analyses per year. Several customers soon
operated the AutoChemist in multi-shifts.
4 Applications
The AutoChemists were used in a variety of
laboratories varying from health screening
centres such as BUPA in London [38-41] and
Kaiser Permanente in San Francisco, to university hospitals such as Odense in Denmark
[42] and Toulouse [43] and Nancy in France,
as well as regional hospitals in Sweden and
Italy and commercial laboratories in Sweden,
the US [44-46], and Japan [47-48].
The first AutoChemist for the US was delivered to the Kaiser Foundation/Multi-Phasic Clinic, Oakland, California, in December
1967 and attracted worldwide interest.
The second installation of three units
started some months later at the United Medical Laboratories (UML) in Portland, Oregon
[44-45]. Another unit was later installed with
all four units running in two shifts. The UML
Lab News claimed in March 1969 [44] that
they were the world’s largest and most automated laboratory. After more than two and a
half years of research, the scientific staff of
UML found in Sweden a revolutionary computer-controlled 30-channel mass testing
system. UML’s Operations Vice-President
defines it as “An automatic analytical device
designed with unusual flexibility for largescale processing of discrete or completely
chemically isolated samples – an analyzer
which is one of the most precise pieces of
automated equipment ever made, having a
built-in monitoring system which practically
eliminates the possibility of error”[44].
The next two units were installed in
1970 at the Metropolitan Laboratory Inc.
(MetPath), New Jersey. MetPath called
their AutoChemist-panel “Chem-Screen”
which involved about 26 tests. In 1975, they
performed close to 1.6 million screens with
about 40 million analyses or > 100,000 per
day. MetPath continued to expand and in
1978 they opened a large new laboratory
in nearby Teterboro [46]. MetPath had ten
AutoChemists, which later even increased
to 11. Their Annual report for 1980 stated:
”The capacity is now 12,000 Chem-Screen”
or around 300,000 tests per day which means
above 100 million tests per year. “MetPath is
the largest clinical laboratory in the world”.
Japan was the first non-Swedish country
showing an interest for the AutoChemist, as
soon as in 1965. Japan Medical Laboratories
(JML) ordered the first AutoChemist in the
early 1970s. The first unit was installed in
Osaka, and later three more at JML, two
in Kyushu and one in South-Osaka. The
head of the Osaka laboratory, Dr Masao
Wakabayashi, was not only interested in test
results but also in the technical solutions.
The AutoChemist concept [47-48] was wellknown in Japan with more than 35 published
articles (1977).
Conclusions
The vision and the ideas of the Jungner
brothers from the early 1960s to construct a
unit both for mass analyses /health screening/ and batteries of analyses in hospitals
were actively debated in Sweden by persistent detractors and keen supporters.
The idea has shown to be of high public health importance, but original units
were not of acceptable size for customers.
This work resulted in a smaller and lighter
version, the AutoChemist-PRISMA® (PRogrammable Individually Selective Modular
Analyzer) [49-50] and as of 1976 it became a
successor for many AutoChemist customers [34]. Companies such as MetPath bought as
many as fifteen of these.
In summary, during the short time in
which the AutoChemist was developed and
operated in numerous locations around the
world, it had a significant impact on the nature and operation of automated equipment
in clinical laboratories. The demand for
robust components capable of continuous
operations for days, based on bulk reagent
preparation and delivery, with innovative
features of on-line monitoring and quality
control, established new standards of operation for clinical laboratories and industry
to meet. Overall, 31 AutoChemists and 44
AutoChemist PRISMA with one to three
modules were sold worldwide.